Abstract: Healthcare is a Fundamental Right
I believe that healthcare is a fundamental right and should be accessible to all, inclusive of all services from preventive, to primary, all the way to tertiary. It is not a privilege that is given only to those who can afford it. Yet, our current health delivery system in the Philippines is just that. It is largely driven by private forces aimed at maximizing their profit. In return, the public healthcare delivery structure is suffering due to inefficient distribution of resources, which in the long run is unsustainable.
Inefficiency is a plague on every human designed system and the Philippine healthcare system is no exception. Now imagine a world in where the delivery of healthcare is of the highest quality and accessible to all. It may seem like an impossible vision relative to our current state. I believe this can be made into a reality with our current technology and healthcare knowledge. Not only is it possible, this universal healthcare system is necessary for our sustained survival and growth as a nation.
Organization: Research-based Centralized Referral System
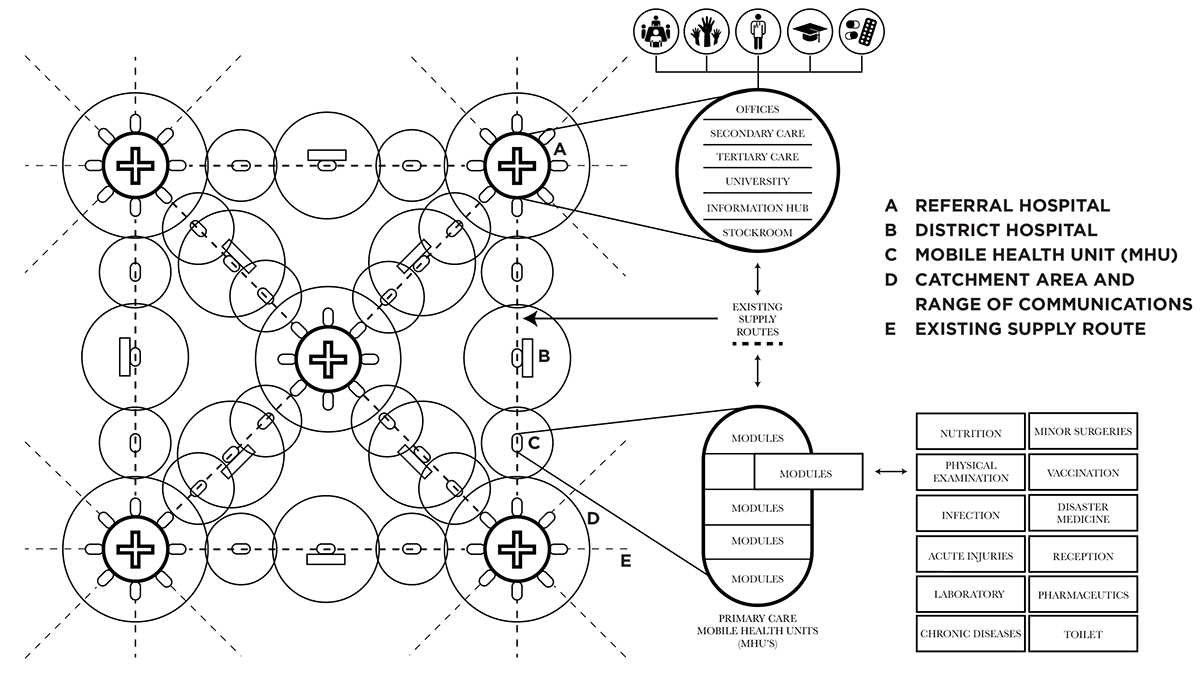
The proposed designed healthcare system is a research-based centralized referral system, in contrast to the current commerce-based centralized system. The healthcare delivery system has a web structure, consisting of three main levels: central, intermediary, and peripheral.
The central level includes the central directorates and programs of the Department of Health, and the Regional Referral Hospitals. It elaborates policies and strategies, ensure proper monitoring and evaluation, and the regulations within the entire health sector. Regional Referral Hospitals are the final sector and are equipped to deal with highly specialized medical scenarios. The intermediary level is found at the Provinces and are operated by the first level LGU’s. It consists of an administrative office that deals with management and policy issues but is not a provider of health services. The peripheral level is represented by the Provincial Hospitals, District Hospitals, Mobile Health Units (MHU’s), and the Barangay Health Workers (BHW’s). Each sector of the peripheral level is given a range of autonomy to deal with health problems of its target population.
An organic healthcare system that is research-based and is decentralized can react to any scenario including natural disasters and disease outbreaks. A research-based system can distribute its healthcare and treat its patients more efficiently using information and data. Due to the different levels of autonomy, each sector in the peripheral level can react quickly without have to depend on the intermediary and central levels.
There is a clear hierarchy of decisions made within each level of healthcare providing clarity and accountability. Decision making is also clearly identified with different levels of authority. Proper capital and information infrastructure must be in place for effective implementation of designed system.

Infrastructure System
The designed infrastructure system is paralleled with the organization of the healthcare system, with a clear hierarchy of responsibilities and a referral system. It also involves an organic structured organization, which allows for expansion and natural growth dictated by supply and demand. It is modular allowing for different permutations of service delivery based on health needs of a community. The different infrastructure typologies within the system include: Regional Hospitals, Provincial Hospitals, District Hospitals, and the Mobile Health Units (MHU’s).
As previously mentioned, Regional Hospitals are responsible for providing tertiary care for the entire population. They only deal with patients that need the most specialized treatment, who are referred by the Provincial Hospitals. Provincial Hospitals are equipped with both secondary and tertiary care, who receive patients from the District Hospitals. District Hospitals on the otherhand are equipped with both primary and secondary care.
Primary care within the District Hospitals are composed of modular MHU’s that are detachable and travel on existing supply routes. These MHU’s carry all the necessary supplies and personnel from one District Hospital to another, while serving rural communities in-between. This enables the system to provide equal access to its citizens and eliminate the need to travel for patients. MHU’s are further supported by a network of Barangay Health Workers (BHW).
Adaptive Capacity
Adaptive capacity is defined as the capacity of a system to adapt if the environment where the system exists is changing. It’s a systems ability to adjust to disturbances, moderate potential damage, takes advantage of opportunities, and copes with the consequences of the occurring transformation.
It can be enhanced by: learning to live with change and uncertainty, nurturing diversity for resilience, combining different types of knowledge for learning, and creating opportunity for self-organization towards social-ecological sustainability.
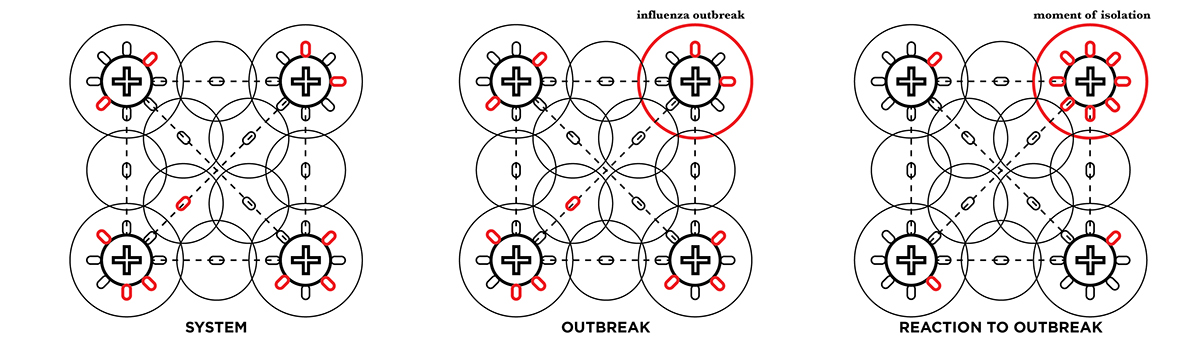
The proposed design has an optimal level of adaptive capacity. It can respond to any scenario as it is both research-based and organic. The two scenarios that healthcare must be most adaptive to is natural disasters and disease outbreaks.
During a natural disaster, medical response time is usually very slow because they have to go through a lot of process. The designed proposal allows for much quicker reaction, due to the inherent modularity and constant motion of the MHU’s.
With the proposed system, when one area get struck and cripples part of the healthcare system, the modular mobile units react and shift towards that one area, where they can then create a semi-permanent health structure. These units are equipped with all the equipment needed for physicians to deliver dignified care, very different to how it is delivered now.
Mobile units also empower system to prepare for natural disasters. Especially now where weather can be predicted to a certain extent, health system can brace for the impact of a natural disaster by removing units from the main hospital decreasing loss of equipment.
There is gap between a natural disaster and full recovery that is often overlooked by disaster relief planners and volunteers. Relief is important to preserve the lives of those afflicted but sustainability is just as important. The context for this project is in that gap between relief and full recovery, in terms of both disaster medicine and Primary Health Care.
These mobile units are surplus of the medical nodes, so function of the hospitals and clinics will not be affected. The only ones that will lose out on medical care during a natural disaster are those in rural areas that the mobile units treat.
Main issues and concern during a natural disaster according to medical professionals revolve around security, communication, potential outbreaks, and transportation. With the proposed organic health system which has an existing chain of command and communications, donations and relief will be more efficiently distributed and accounted for.
Scenario: Natural Disaster

Similar to the natural disaster scenario, the mobile units can move resources to deal with specific issues such as a disease outbreak. This is needed for quick isolation. A lot of issues regarding the current Ebola crisis is the transportation of patients from their village to the clinic. This removes the need of travel.
Scenario: Disease Outbreak
Modular Health Unit (MHU)
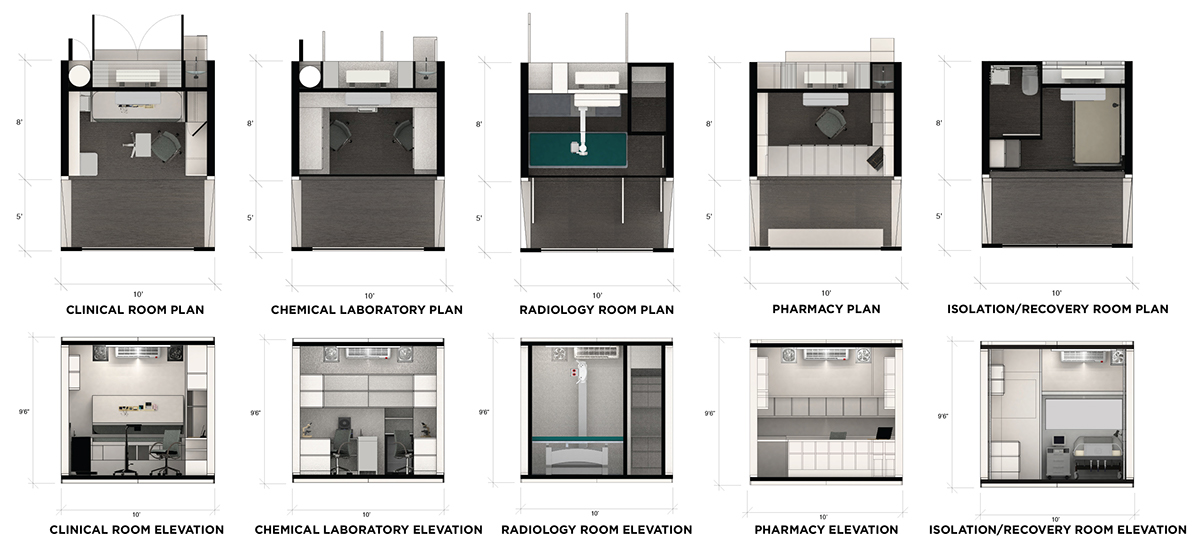
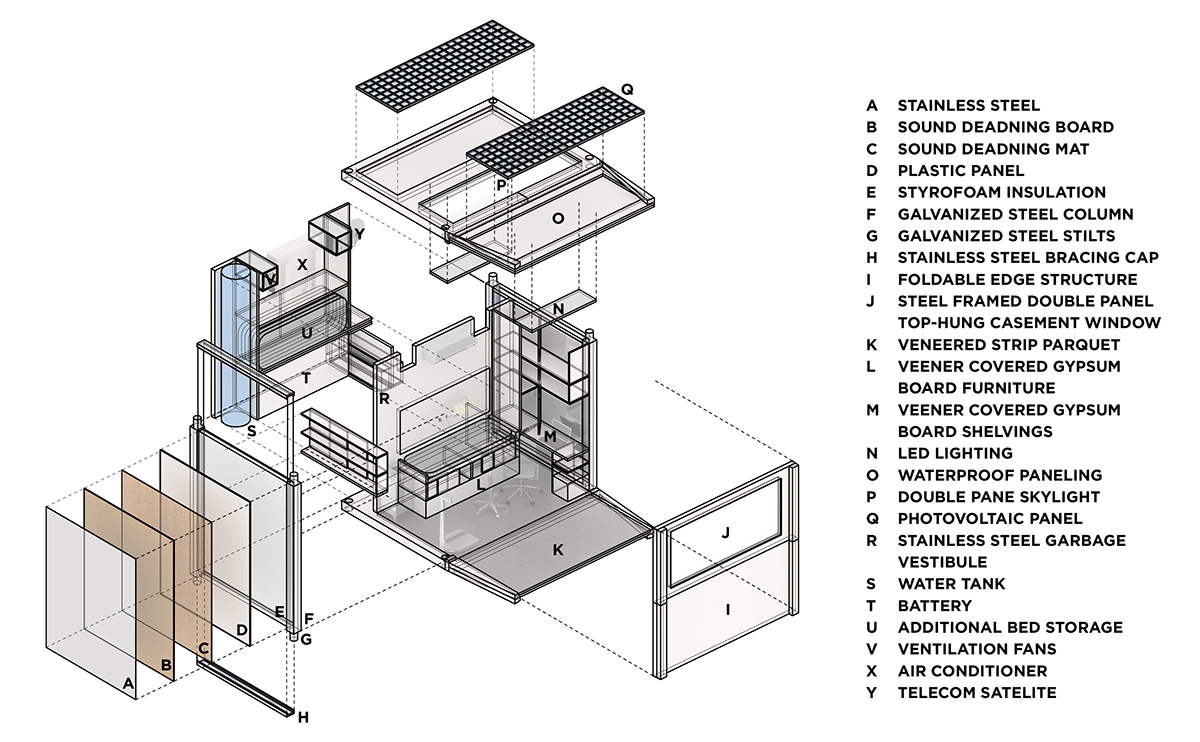
The proposed modular Mobile Health Unit come in two major categories: Independent and Dependent. The independent units have a complete mechanical system including power and water supply, while the dependent units have to rely on the independent units for said provisions. Functionality and comfortability were the main priorities when designing these mobile units.
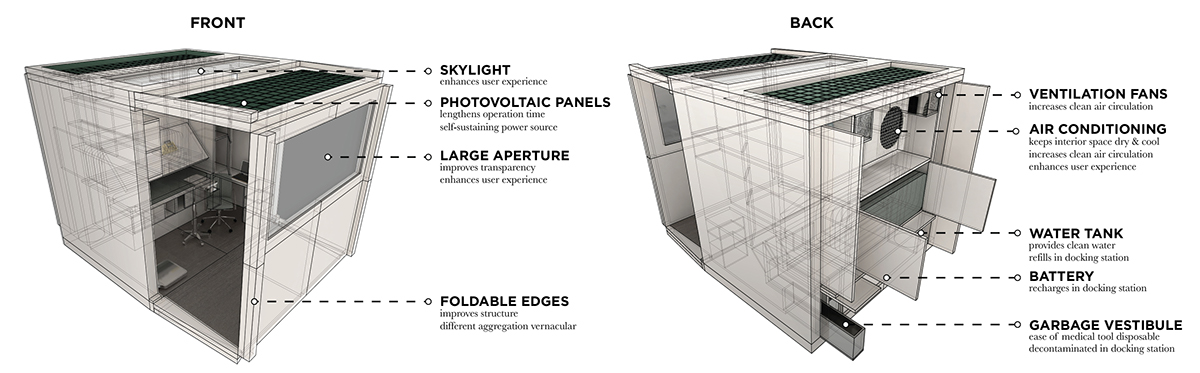
All MHU’s will be equipped with: skylights to enhance user experience, photo-voltaic panels to lengthen operation time, large apertures to improve transparency and enhance user experience, foldable edges to improve structure and create different aggregation vernacular, ventilation fans to increase air circulation, air conditioning to keep interior space dry and cool which increases user experience, water tank to provide clean water, battery that recharges at the docking station, and a garbage vestibule that is decontaminated in a docking station which resolves hazardous waste.
The proposed modular Mobile Health Unit come in two major categories: Independent and Dependent. The independent units have a complete mechanical system including power and water supply, while the dependent units have to rely on the independent units for said provisions. Functionality and comfortability were the main priorities when designing these mobile units.
All MHU’s will be equipped with: skylights to enhance user experience, photo-voltaic panels to lengthen operation time, large apertures to improve transparency and enhance user experience, foldable edges to improve structure and create different aggregation vernacular, ventilation fans to increase air circulation, air conditioning to keep interior space dry and cool which increases user experience, water tank to provide clean water, battery that recharges at the docking station, and a garbage vestibule that is decontaminated in a docking station which resolves hazardous waste.
Unit Transportation
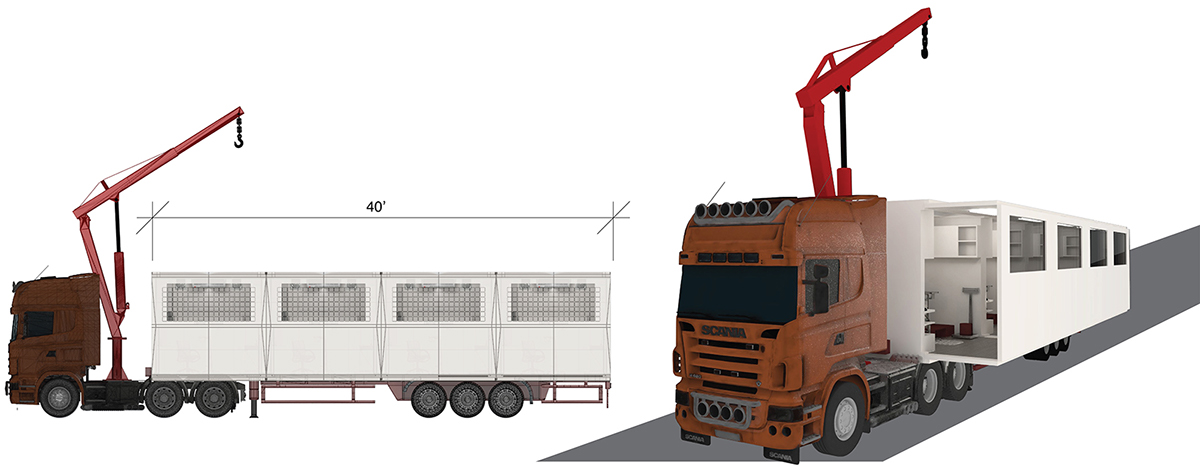
Since dimensions are derived from conventional ISO containers, units can be transported in multiple ways which leads to its flexibility. Mobile units can be transported through traditional cargo ships, cargo planes, helicopters, and land vehicles. However, for this system they will mostly be transported using land transportation due to cost and convenience. The maximum length of a cargo truck can carry 40 feet, a total of 4 different modular mobile units. If needed, mobile units can be deployed on site either on top of the truck, or aggregated on the ground.
Rural Area Unit Aggregation Type 1
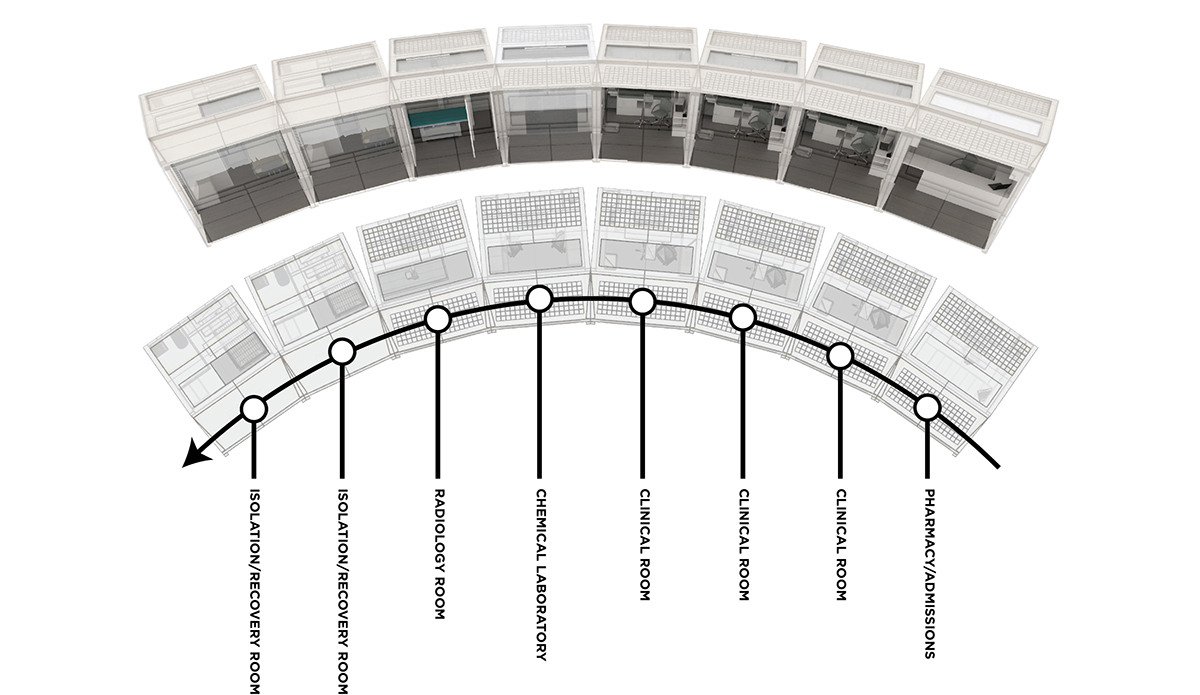
The first type of aggregation is made possible due to the designed foldable edges. According to research, monotonous paths are detrimental to the recovery of a patient. Undulating forms and wave motion, like nonlinearity is crucial and omnipresent in nature, which has proven to hasten patient recovery. The curved path allows patients to engage with the architecture more actively.
This type of aggregation is designed for small demand areas or areas with planned healthcare where a waiting area is unnecessary. It can continue to aggregate and create a Panopticon, which is a circular structure with a radial organization.

Rural Area Unit Aggregation Type 2
The second type of aggregation takes advantage of the folding doors to create a wide hallway from the negative space in-between units. This type of aggregation is optimal for larger demand areas in where transparency is essential. Since units are facing each other, nurses and doctors can respond to emergency situations quicker. The transparency leads to optimization of the system and decreases amount of needed practitioners on site. Large hallway can also be used to house the waiting room or can be made to a recreational space.

Logistical Narrative for Mobile Unit
Diagram portrays the daily schedule and route of a mobile unit from the Hospital to the Rural Area to the Clinic. There are two daily shifts and routes in where units are deployed from hospital to clinic and vice-versa, one in the morning and the other in the afternoon. During morning deployment, health units in rural areas on route are replenished or replaced including medical supplies and doctors. They are then either removed or the doctors are picked up on the afternoon route. Diagram also traces all personnel involved with each action, which shows that minimal amount of additional staff are needed to run the system.

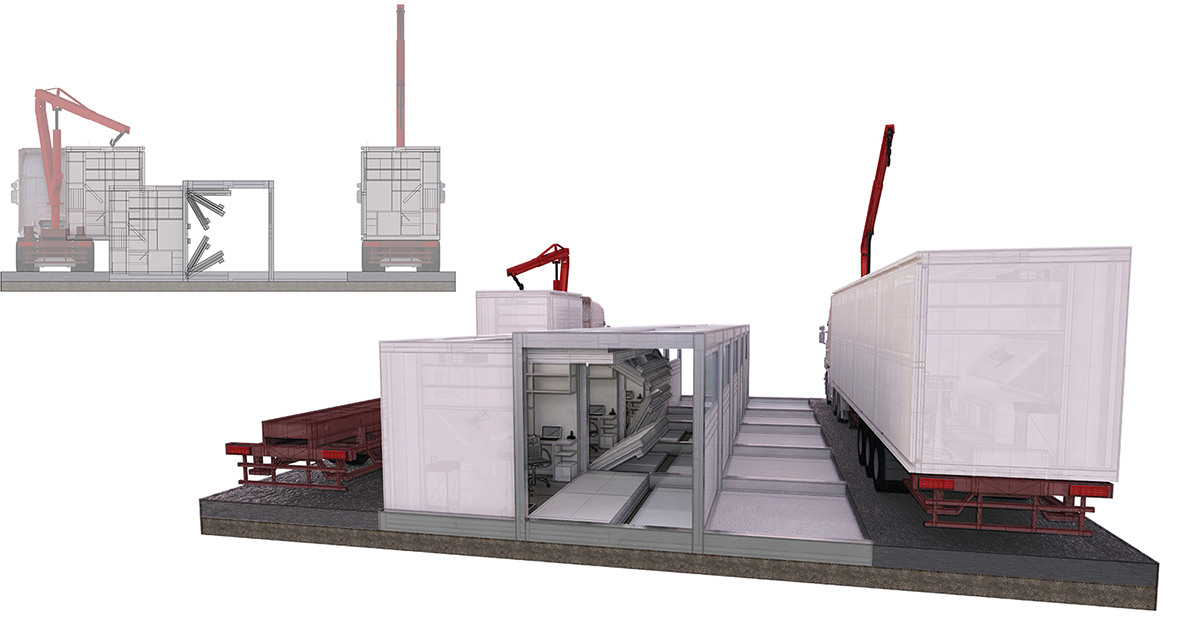
Docking Sequence
Units are unloaded from the trucks using a crane and fit into a designed void for accuracy. The doors of the units then unfold in synchronization with the doors of the docking station structure. Folding doors are important to maintain sanitation and cleanliness of areas when units are docking. Windows are also placed specifically to provide an aperture for the photovoltaic panels to receive sunlight when docked. Mechanical resources such as electricity and water of units are replenished when docked in either the clinic or the hospital. Layout of mechanical follows the layout of the corridor which leads to endless growth.

Modular District Hospital Design
In accordance to the entire healthcare structure, the designs for the larger healthcare infrastructure are composed of MHU’s that provide it’s primary care services. The structure of the District Hospitals are based on how the MHU’s aggregate and the way they dock. Therefore, the same design principle of modularity is also applied. They are all units to a whole. Due to its modularity, it can grow and expand depending on the need of its population.
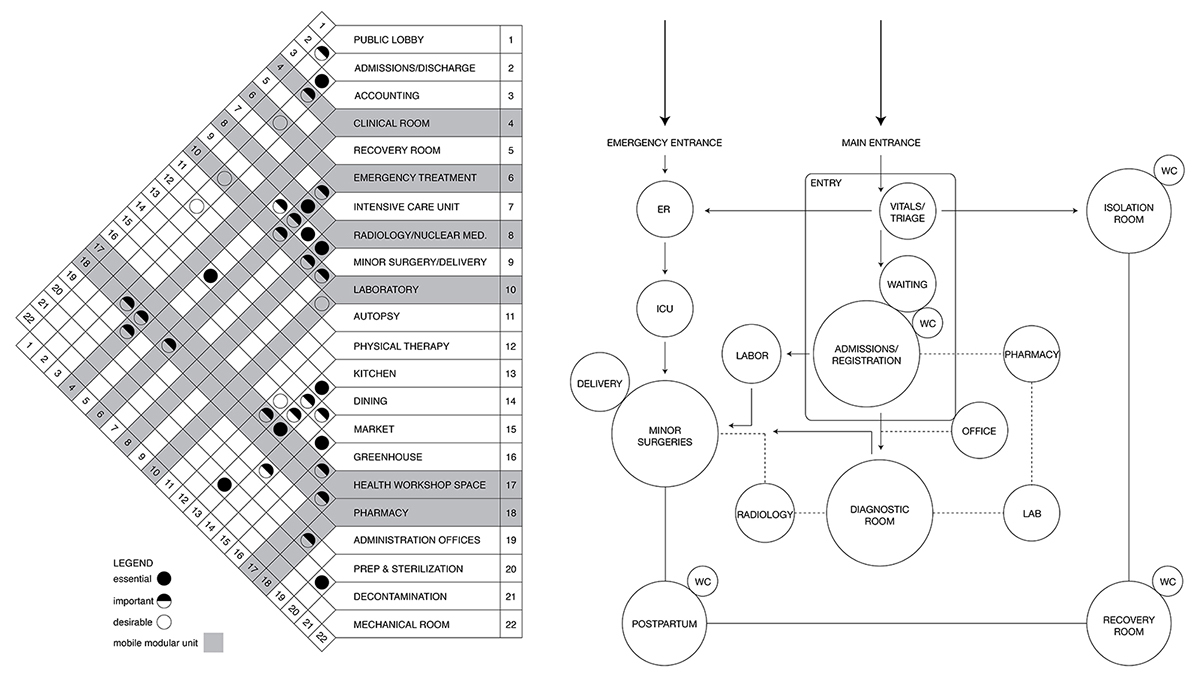
Program Matrix
Apart from the standard program of the District Hospital as mentioned earlier in the typologies, additional design constraints include fluid growth and expansion. The standard program matrix for a District Hospital was used and then the adjacency of the MHU’s were added, which shaped the flow and layout of the program. Additional program such as a restaurant, a market, a greenhouse, and a health workshop space, add focus on preventive health care.
Triage Flow
The triage flow chart shows the same adjacency of the program matrix in terms of patient process. District Hospital has two main entrances: Emergency and Main, which leads to two different sequences. Vitals and triage are at the forefront of the process to prioritize segregation of patients, which is important for areas with high amounts of infectious diseases such as tuberculosis, like in the Philippines.
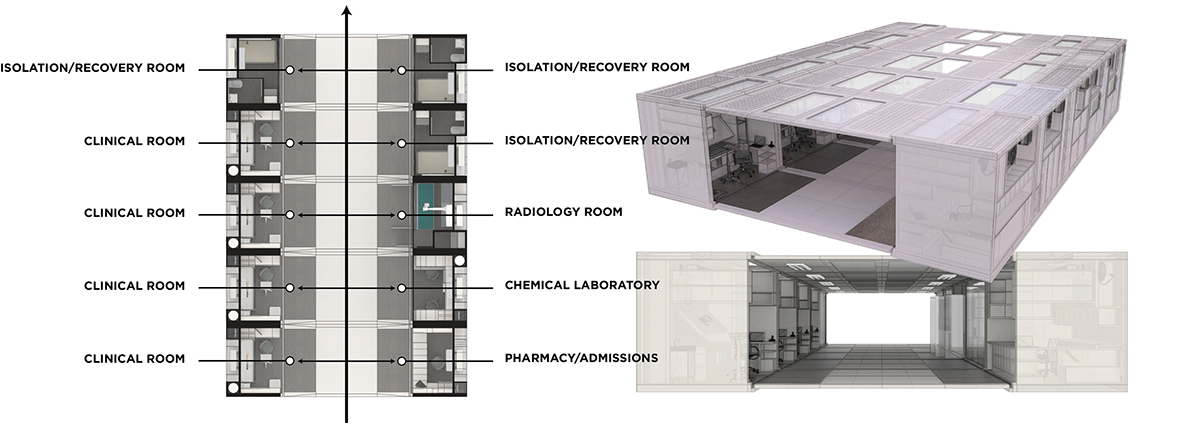
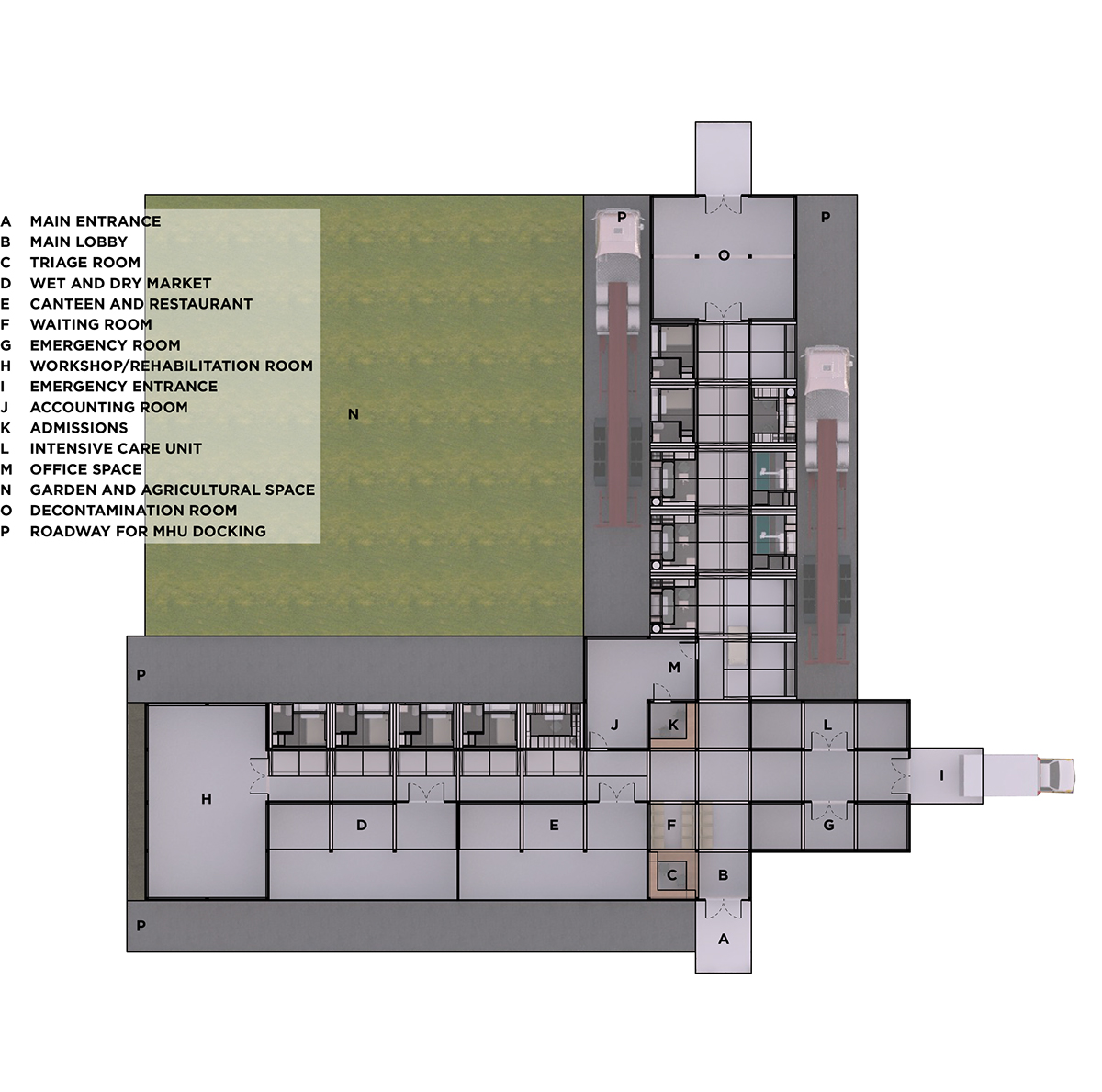
Program Layout
Both the program matrix and the triage flow chart is transformed to create the program layout. The proposed clinic design has a two-axis corridor and is divided between diagnoses, intensive care, and recovery areas. Intensive care has its own entrance where ambulances can park without obstruction. Recovery area includes a recreational room, restaurants, and markets to promote patient engagement leading to quicker health recovery. Both the views from the isolation room, and the recovery room are directed towards the garden and courtyard which has proven to hasten health recovery as well.
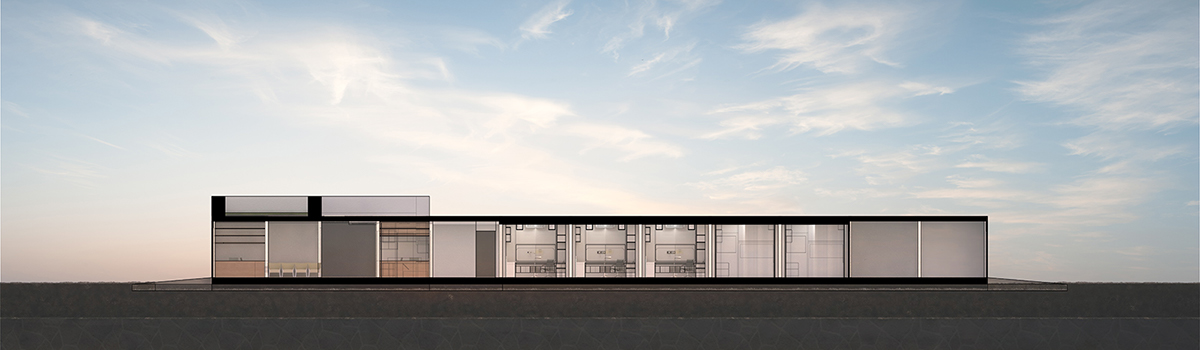
District Hospital Section A
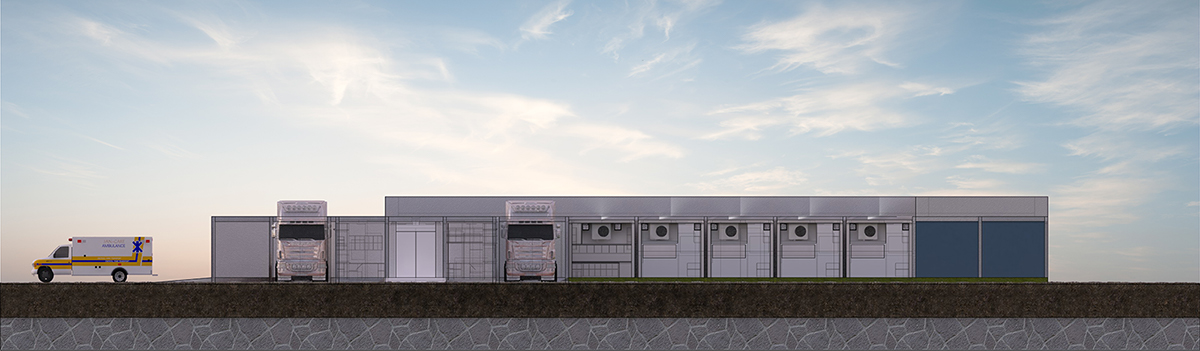
District Hospital Elevation
Patient Health Driven Design
It is important to have a standardized set of construction guidelines to maintain accountability and ease of construction. However, it is also vital to design a sense of community within the design. Successful medical facility design in part hinges on its ability to contribute to a community’s sense of place, its genius loci. By engaging the community through shared garden space, markets, and restaurants, the clinic has the ability to define its own unique identity through cultural and vernacular qualities.
Therefore, design for the District Hospital is not only organic for the way it is structured but leaves space for the unstructured growth of a community and an identity. Large skylight in the lobby to establish institutional identity and a place for people to enter and spend time rather than simply a space to rush through to reach another destination point.
District Hospital design includes a vast garden and courtyard with direct experience for patients. Unstructured contact with self-sustaining attributes of the natural non-human built environment hastens patient recovery.Roof incorporates a therapeutic garden, rainwater harvesting for cultivating vegetables, and photovoltaic panels; all important for both the health of the patient and of the building.



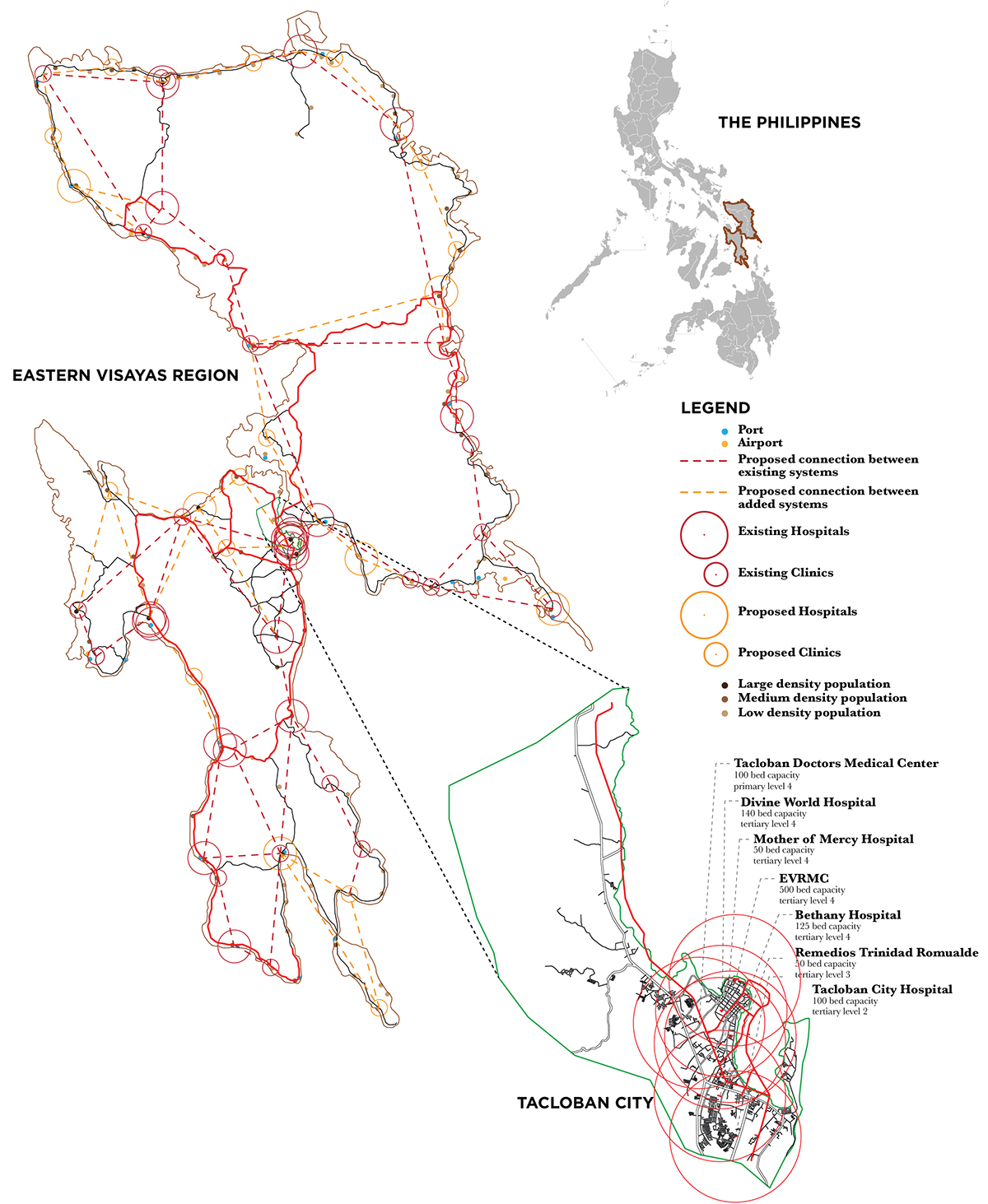
Context Simulation: East Visayas Region, Philippines
Eastern Visayas Region in the Philippines is the context chosen to simulate the proposed Organic Healthcare System.
One of the main cities in the Eastern Visayas Region is Tacloban, which has a population of 220 thousand people. It has 7 hospitals that range from primary to tertiary care that houses a total of 1065 beds. With a ratio of 1 bed per 208 people, it is five times the average of the Philippines of 1 bed per 1000. However, this does not portray a complete picture of the health environment in the region. Looking at the medical environment on a regional scale, it is clear that there is large disproportion regarding the distribution of medical facilities.
Last year, they experienced a natural disaster that crippled their entire health system which disabled them to treat for much needed acute injuries. They were not prepared to deal with a situation like this and a lot suffered for it. Even the airport was turned into a temporary health clinic due to heavy demand. Top 5 consultations include URTI, Headache/dizziness, wounds, hypertension, and musculoskeletal pain.
The proposed system was then projected with the region’s existing hospitals and clinics within the region by creating a network through main highways. Based on intense research on the site, additional hospitals and clinics are proposed depending on demand and existing health issues.
While mapping, it is made evident that there were a large amount of the population who do not have access to health care, which the modular mobile unit addresses. In the more rural areas of Tacloban, the civilians rely on a self-supporting community health program backed with common agricultural goods.
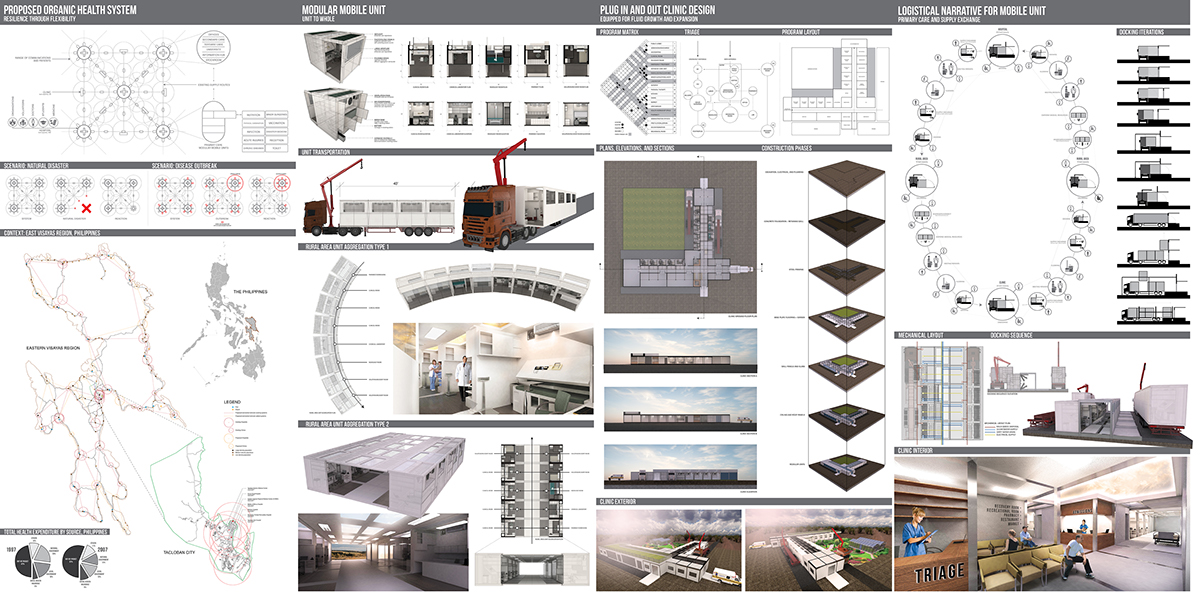
Presentation Board: